

Resources for Communication Problems

Showing posts with label NC14. Show all posts
Showing posts with label NC14. Show all posts
Thursday, March 13, 2008
NC299S14
NC299S14
Chapter 14 Motor System 4 : Motor Cortex
The several motor cortices control voluntary manipulative and delicate motor movements and initiate motor performance. Descending cortical projections to the motor neurons travel via two pathways, the corticobulbar tract and the corticospinal tract, collectively called the pyramidal tract. These tracts control cranial and spinal motor neurons (LMN), respectively. Activity at the motor cortex is influenced by extensive feedback channels from the cerebellum, brainstem, thalamus, and basal ganglia.
不同的運動皮質支配隨意操縱和精巧靈敏的動作以及執行運動的開端。 下行皮質投射至運動神經運行經由兩個路徑,corticobulbar tract和大腦皮質脊髓徑,總稱錐體路徑。這些路徑個別控制腦和脊髓運動神經。運動皮質的活動受小腦、腦幹、視丘、及基底核的回饋通道影響非常大。
A lesion interrupting the excitatory projections from the motor cortex results in a specific loss of delicate motor control. It also results in sings of muscle weakness, flaccid tone, hyporeflexia, and loss of reflexes. However, in several weeks, the hyporeflexia and flaccid tone are replaced by increased reflexes (hyperreflexia ) and spastic tone in muscles.
若有一傷害打斷運動皮質的刺激將會很明顯的造成精細運動的控制喪失。 也會造成肌肉無力、肌肉張力下降、反射減弱、甚至反射作用喪失。然而在幾週內,反射減弱和肌肉張力下降會轉變為反射過強以及肌肉痙攣的現象。
Friday, January 25, 2008
NC299TT Chapt.14
NC299TT Chapt.14
NC299TT01
負責人:9580022 承樺
Alternating hemiplegia
交替的半身不遂
Alternating hemiplegia is a rare condition where a child has episodes of weakness affecting one side of the body. This weakness can affect all the muscles on the affected side, not just those in the limbs. After an episode, the weakness improves, but will recur during the next episode. Alternating hemiplegia is a variable condition that affects children to differing degrees and in a variety of ways. This can make it a difficult condition to diagnose and manage but much expertise has been gained in recent years.
Alternating hemiplegia is a condition which has transient weakness of either, or sometimes both, sides of the body. The attacks may alternate or sometimes overlap, that is the second side is affected before the first recovers. Attacks start in the first year of life and are often accompanied by unusual irregular eye movements. The attacks last from less than an hour which is unusual to sometimes several days. When the attacks are prolonged the manifestations are not apparent during sleep or for the first fifteen to twenty minutes on waking when they then return. This is a very characteristic finding and when there are bilateral attacks this may allow feeding and drinking to occur in that short clear period after waking. The episodes of hemiplegia are not epileptic in nature but epileptic seizures may co-exist and require separate anti-epileptic drug treatment.
The cause is not known. Affected children usually have significant learning disabilities and motor organisational problems, including unsteadiness. There is a tendency for these problems to increase with repeated episodes.
Treatment is with flunarizine (a calcium channel blocker). Other drugs have not been found to be consistently helpful.
來源:http://www.ich.ucl.ac.uk/factsheets/families/F060393/index.html http://www.cafamily.org.uk/Direct/a39.html
NC299TT02
負責人:9580023 嘉芸
Babinski reflex
巴賓斯基反射
一種神經性測試方法, 顯示異常的足底反射, 表示中樞神經系統發生損害
extension upward of the toes when the sole of the foot is stroked firmly on the outer side from the heel to the front; normal in infants under the age of two years but a sign of brain or spinal cord injury in older persons.
An extension of the great toe, sometimes with fanning of the other toes, in response to stroking of the sole of the foot. It is a normal reflex in infants, but it is usually associated with a disturbance of the pyramidal tract in children and adults. Also called Babinski sign, Babinski's sign.
NC299TT03
負責人:9580024 寬哲
Corticobulbar tract
大腦皮質與延髓的通道
Corticonuclear tract is a white matter pathway connecting the cerebral cortex to the brainstem (the term "bulbar" referring to the brainstem).
NC299TT04
負責人:9580025 宜蒨
corticospinal tract
皮層脊髓束
NC299TT05
負責人:9580026 鳳徵
cremasteric reflex
提睪肌反射
Retraction of the testicle on stroking the skin of the inner thigh. Absence of this reflex indicates a pyramidal tract lesion (upper motor neuron).
睪丸的收縮在於撫摸大腿內側的皮膚。缺乏此反射象徵一種椎狀體路徑機能障礙。
相關網站:http://www.ohayoo.com.tw/%B3J%B3J%A9%BF%B5M%A4%A3%A8%A3%A4F.htm
相關圖片:http://content.answers.com/main/content/wp/en/thumb/c/c9/250px-Layers_of_the_scrotum.gif
{kind=link}
NC299TT06
負責人:9580027 子倫
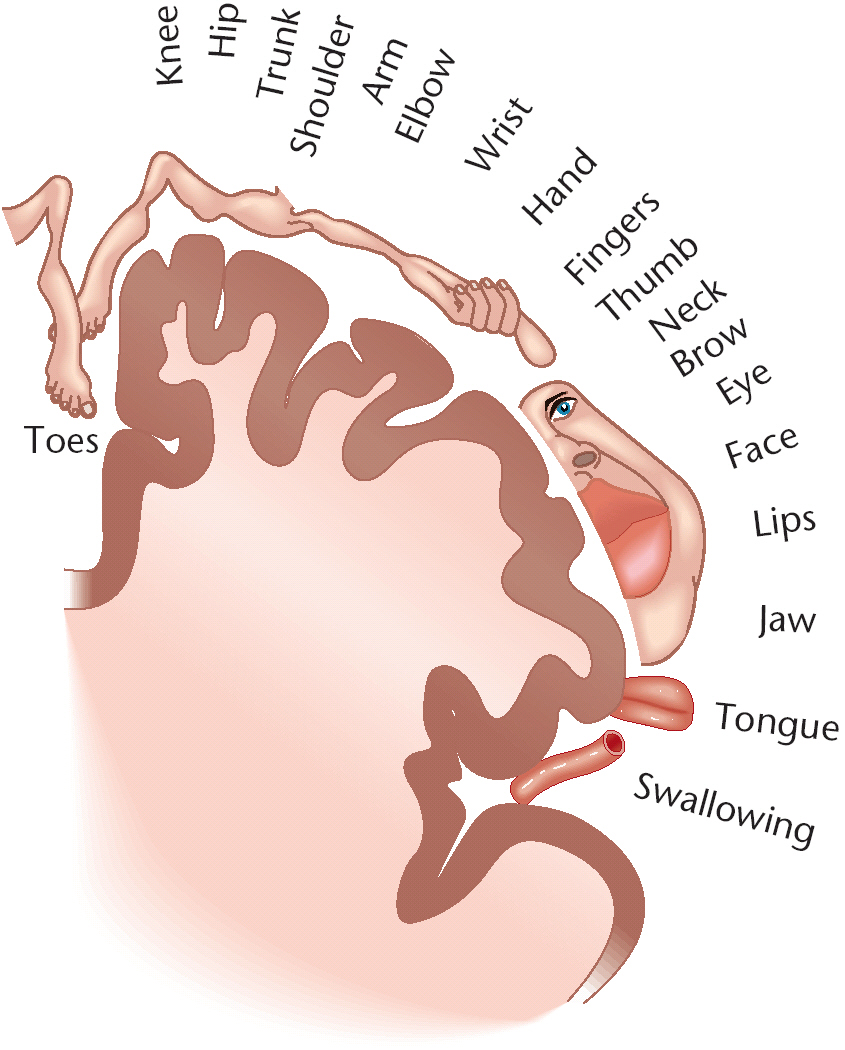
homunculus
homunculus Representation of the body in the sensorimotor cortex. 身體呈現在感覺運動皮質區。術語翻譯:小型人類(身體很小各部分成比例與一般侏儒不同) 圖片補充: http://spinacare.files.wordpress.com/2007/02/homunculus.jpg
{kind=link}
NC299TT07
負責人:9580028 曣晴
從缺
NC299TT08
負責人:9580029 姵妏
從缺
NC299TT09
負責人:9580030 欣玉
premotor cortex
前運動皮質區
大腦皮質負責許多「高等」的認知功能,像是語言以及訊息處理。分成好幾個功能區,此為其中一個。
參考資料:http://tw.knowledge.yahoo.com/question/question?qid=1405111220210
NC299TT10
負責人:9580031 建宇
pyramidal decussation
錐體交叉
錐體徑的大部份纖維在Medulla oblongata (延腦)下緣與脊髓交接處交叉到對側,這個交叉處稱為錐體交叉。
補充:
<一>錐體位置與組成
Medulla oblongata(延腦) 下方和脊髓相連以Foramen magnum (枕骨大孔)為界。上方和Pons(橋腦)相接連。Medulla oblongata 腹側中線處有一對Pyramid (錐體),內部由皮質脊髓徑所構成。
<二>Decussation of pyramid (錐體交叉):
1.錐體徑的大部份纖維在Medulla oblongata (延腦)下緣與脊髓交接處交叉到對側,這個交叉處稱為錐體交叉。
2.Medulla oblongata 內部有 5對腦神經核(CN.8~12),即:位於Medulla oblongata (延腦)前面中間二側是Pyramid (錐體)
CN.8:Vesiulocochlear n. (前庭耳蝸神經)的Cochlear n (耳蝸枝)
CN.9:Glossopharngeal n. (舌咽神經)
CN.10:Vagus n. (迷走神經)
CN.11 Accessory n. (副神經)
CN.12 Hypoglssal n. (舌下神經)
※除了CN.8於延腦-橋腦交接處的橋延溝進入外,餘皆由Medulla oblongata進出。
3.Olive (橄欖核)後方由上而下有: CN9 Glossopharngeal n (舌咽神經) 、CN10 Vaus n (迷走神經)、CN11 Accessory n (副神經)、 Olive (橄欖核),Pyramid (錐體)間有:CN12 Hypoglssal n (舌下神經)
4.管理隨意運動和精細動作的錐體系的錐體細胞位於大腦皮層運動區,其發出的纖維組成錐體束,經腦幹下行,小部分止於腦幹腦神經運動神經細胞,大部分在延腦下段交叉到對側,再下行止於脊髓前角運動神經細胞。腦神經軀體運動纖維分佈到頭面等部骨胳肌,脊神經運動纖維則支配軀幹四肢骨胳肌。如錐體束在交叉前受損傷,引起對側肢體肌肉癱瘓;如損傷部位在錐體交叉以下,則表現為患側肢體癱瘓。
5.錐體細胞和錐體束受損傷表現為硬癱,即癱瘓肢體張力增高,腱反射亢進,劃蹠試驗陽性(barbinski’s sign)。腦、脊髓運動神經細胞體及神經纖維受損傷表現為軟癱,癱疾肢體張力低,一切反射消失。軀體感覺纖維也交叉上行,右側大腦皮層感覺區接受來自左側軀體的感覺。
6.錐體外系統
是運動系統的一個組成部分,包括錐體系統以外的運動神經核和運動傳導束,由基底神經節(新紋狀體——尾狀核、殼核,舊絞狀體——蒼白球、黑質)和丘腦底核、紅核、網狀結構等組成,主要調節肌張力、肌肉的調節運動和平衡。錐體外系統損害,可出現肌張力的改變,不自主多動,如帕金森氏綜合征、舞蹈症、舞蹈樣手足抽動症和扭轉性痙攣等。
<三>資料來源:
http://www.hk.edu.tw/~mehu/anatomy%20lab/Nervous%20system/Medulla.htm
<四>單字分解
pyramidal《形》 錐體的;錐狀的.
decussation X形交叉;中央神經系統的交叉神經纖維
NC299TT11
負責人:9580032
Pyramidal tract
錐體徑
由大腦而之神經纖維,經過脊髓至前角運動細胞
NC299TT12
負責人:9580033 筱柔
spastic hemiplegia
痙攣性偏癱,偏癱是指身體的一側半邊發生麻痺癱瘓,原因是腦部的另一邊受到破壞,由於神經在腦部交叉,腦神經的一邊控制身體另一邊的手腳行動,通常是腦中風(stroke)症狀的一種;如果肌肉不是完全癱瘓,則稱為「痙攣性偏癱」
*spastic 痙攣的 *hemiplegia 偏癱;半身不遂.
參考網址:http://www.ultraflexsystems.com/firstflex/patients/
NC299TT13
負責人:9580035 婷婷
Supplementary motor cortex
輔助運動皮質
大腦造影技術的進步,讓我們可以觀察到動作控制或者學習過程中大腦腦區之間的活化型態,透過對不同動作引起大腦活化型態的差異,了解他們之間特性的不同。例如,新奇或是複雜的動作會引起前運動皮質區( premotor cortex )的活化;但是,當動作熟練後這區就靜止下來,反而是內側的輔助運動皮質( supplementary motor cortex )趨明顯活化。從大腦的動作訊息處理方式及腦部弁鄐幫洠茯搳A額葉型他手症由於受傷位置在對側內額葉及胼胝體的位置,外前運動皮質區由於同側的及對側輔助運動皮質區抑制解除過度活化,因此只要有外在刺激就會不自主的出現動作。
參考資料:http://www.nfapt.org.tw/bimonthly_detail.php?id=1289&vid=83
NC299TT14
負責人:9580036 郁文
Upper motor neurons (UMNs)
上運動神經元
Cell bodies in the motor cortex and their descending axonal processes that synapse on the cranial and spinal motor neurons.
上運動神經元的細胞體主要位於大腦皮質體運動區的錐體細胞,這些細胞的軸突組成下行的錐體束,其中下行至脊髓的纖維稱為皮質脊髓束;沿途陸續離開錐體束,直接或間接止於腦神經運動核的纖維為皮質核束。
http://disable.yam.org.tw/resource/life/als/ch07.htm
NC289L Chapt.14
NC289L Chapt.14
NC289L 01德立
Discuss the motor roles of the primary motor cortex and surrounding cortical areas
討論運動作用主要的運動皮質和周圍皮質區域。
資料在課本的P289,P290,P291,P292 Figure 14-1,14-2,14-3
NC
Outline the anatomic organization of the primary motor cortex.
略述主要動作皮質的解剖組織
you can find the answer at P.289~290
NC289L 03何宏祥
Describe the functions of the corticospinal and corticobulbar pathway
描述脊髓皮質和延髓皮質路徑的功能
Find anatomical pictures for corticospinal and corticobulbar pathway
在NC291~NC293可以獲得答案
在NC
皮質脊髓分為兩種:外側皮質脊髓徑:是將運動性衝動由大腦皮質之一側傳至對側脊髓的灰質前角,最後衝動抵達身體對側的四肢遠端骨肌,協調精確並有技巧的運動;前側皮質脊髓徑:是將運動性衝動由大腦皮質之一側傳至 "同" 側脊髓在交叉至 "對側中軸及四肢近端骨肌", 維持肌肉緊張度與姿勢的控制
皮質延髓徑:顏面運動的控制是由大腦額葉皮質經由皮質延髓徑下行,然後交叉至對側位於橋腦的顏面神經核,再經由顏面神經,控制臉部表情
NC
Discuss the bilateral cortical innervation of speech-related cranial nerve nuclei
討論和說話相關的神經核兩邊腦皮質區神經分配
可在P289~P292找到
NC289LO5曾琦喻
Describe the location of upper motor neurons
形容上部動作神經元的位置
答: 可以在p.291~293頁找到相關內容還可以參考Box14-1
NC
Differentiate between upper motor neuron and lower motor neuron syndromes
_____上行運動神經和下行運動神經的神經症候群的不同
Upper does not mean go upward, lower does not mean go downward. The difference is in location, not in direction of conduction / transmission
可能出現處.292-295 296T14-1
NC
Explain the pathophysiology of spastic hemiplegia
解釋麻痺性半身不遂的病理生理學
ð P.293 可找到
NC
Discuss the pathophysiology of alternating hemiplegia and describe its clinical symptoms.
討論交替的偏癱病理生理學和描述它的臨床症狀。
可以參考課本NC294和NC295還有圖14-4。
NC
Explain the physiology of intact emotional responsiveness in pseudobulbar palsy.
解釋在假延腦病癱瘓中,生理上完整的情緒的敏感度。
intact emotional responsiveness means the patient’s emotional response is basically OK.
答案在P.294可以找到。
NC
Discuss the pathopysiology of alternating hemipegia and describe its clinical symptoms
討論交叉性偏癱(兩側均有症狀,唯重輕不同,上下不同,如:一邊在面,一邊在上肢,病灶在延髓下部)的病理生理學及描述其臨床上的症狀。
相關資料可在課本p294-296、Figure14-4,14-5,14-6找到。
Subscribe to:
Posts (Atom)